Recall(So far in this series)
The first five hallmarks describe a cell that grows autonomously, ignores stop signals, resists death, replicates indefinitely, and has built itself a blood supply. Hallmark #6 is the one that makes cancer lethal in most cases — the ability to leave, travel, and establish itself somewhere else.
Approximately 90% of cancer deaths are caused not by the primary tumor but by metastasis. A tumor confined to its organ of origin is usually manageable — surgically removable, or at least containable. A tumor that has spread to liver, lung, bone, or brain is a fundamentally different clinical problem.
Metastasis is not a single event. It is a multi-step cascade, each step with its own barriers, and cancer cells that complete all of them are a highly selected minority.
The metastatic cascade
Definition(Metastatic cascade)
The sequence of steps required for a cancer cell to successfully colonize a distant organ: local invasion through the basement membrane and surrounding stroma, intravasation into blood or lymphatic vessels, survival in circulation, extravasation at a distant site, and colonization of the new tissue microenvironment.
Each step is a bottleneck. Studies tracking labeled tumor cells suggest that while millions of cells may enter the bloodstream daily from a large tumor, the fraction that successfully establish a distant metastasis is tiny — estimated at less than 0.01%. Metastasis is inefficient, which is why even in metastatic disease, the burden is often concentrated in a small number of sites.
Step 1: Local invasion
The first barrier is the basement membrane — a dense meshwork of collagen IV, laminin, and proteoglycans that separates epithelial tissue from the underlying stroma. Normal epithelial cells can't cross it. Cancer cells that are going to metastasize must degrade and penetrate it.
This requires:
- Matrix metalloproteinases (MMPs) — secreted proteases that degrade collagen and other ECM components. Tumors upregulate MMPs both in tumor cells themselves and in recruited stromal cells (fibroblasts, macrophages).
- Cytoskeletal remodeling — the cell must extend pseudopods and generate the mechanical force to move through tissue
- Loss of E-cadherin — E-cadherin is the adhesion molecule that locks epithelial cells together and keeps them stationary. Its downregulation is one of the earliest and most critical steps in invasion.
Step 2: Epithelial-mesenchymal transition (EMT)
The loss of E-cadherin is part of a broader program called EMT — epithelial-mesenchymal transition — in which epithelial cells acquire the morphology and behavior of mesenchymal cells (the migratory, loosely organized cells of connective tissue).
Definition(Epithelial-mesenchymal transition (EMT))
A cellular reprogramming process in which epithelial cells lose apicobasal polarity, cell-cell junctions (E-cadherin, occludin, claudins), and epithelial markers, and acquire mesenchymal characteristics including vimentin expression, N-cadherin, loss of basement membrane attachment, and migratory capacity. Driven transcriptionally by SNAIL, TWIST, ZEB1/2, and other EMT-TFs. Partially reversible — metastatic colonization often involves the reverse process (MET).
EMT-inducing signals come from the tumor microenvironment: TGF-β (here appearing in its late-stage tumor-promoting role, as previewed in hallmark #2), Wnt ligands, FGF, EGF, and hypoxia all drive EMT transcription factor expression.
A cell that has undergone EMT is invasive, motile, resistant to anoikis (detachment-induced apoptosis), and stem-like. These are precisely the properties needed for the next steps.
Intuition(EMT is a spectrum, not a switch)
Early models treated EMT as a binary — epithelial or mesenchymal. Current understanding recognizes it as a spectrum of intermediate states, often called partial EMT or hybrid E/M states. Cells in a hybrid state retain some epithelial properties (including the ability to cluster) while gaining mesenchymal motility. Circulating tumor cell clusters — which metastasize far more efficiently than single cells — are thought to represent this hybrid state. Pure mesenchymal cells may actually be poor colonizers because MET (the reverse transition) may be required for proliferation at the distant site.
Step 3: Intravasation
Once in the stroma, a cell needs to enter a blood vessel or lymphatic. This requires navigating to a vessel, crossing the endothelial lining, and entering the lumen.
Macrophages play a surprisingly active role here. Tumor-associated macrophages (TAMs) are frequently found at sites of intravasation, and paracrine signaling between TAMs (secreting EGF) and tumor cells (secreting CSF-1) creates a co-migratory program — the macrophage and tumor cell move together toward the vessel, with the macrophage facilitating entry.
Step 4: Survival in circulation
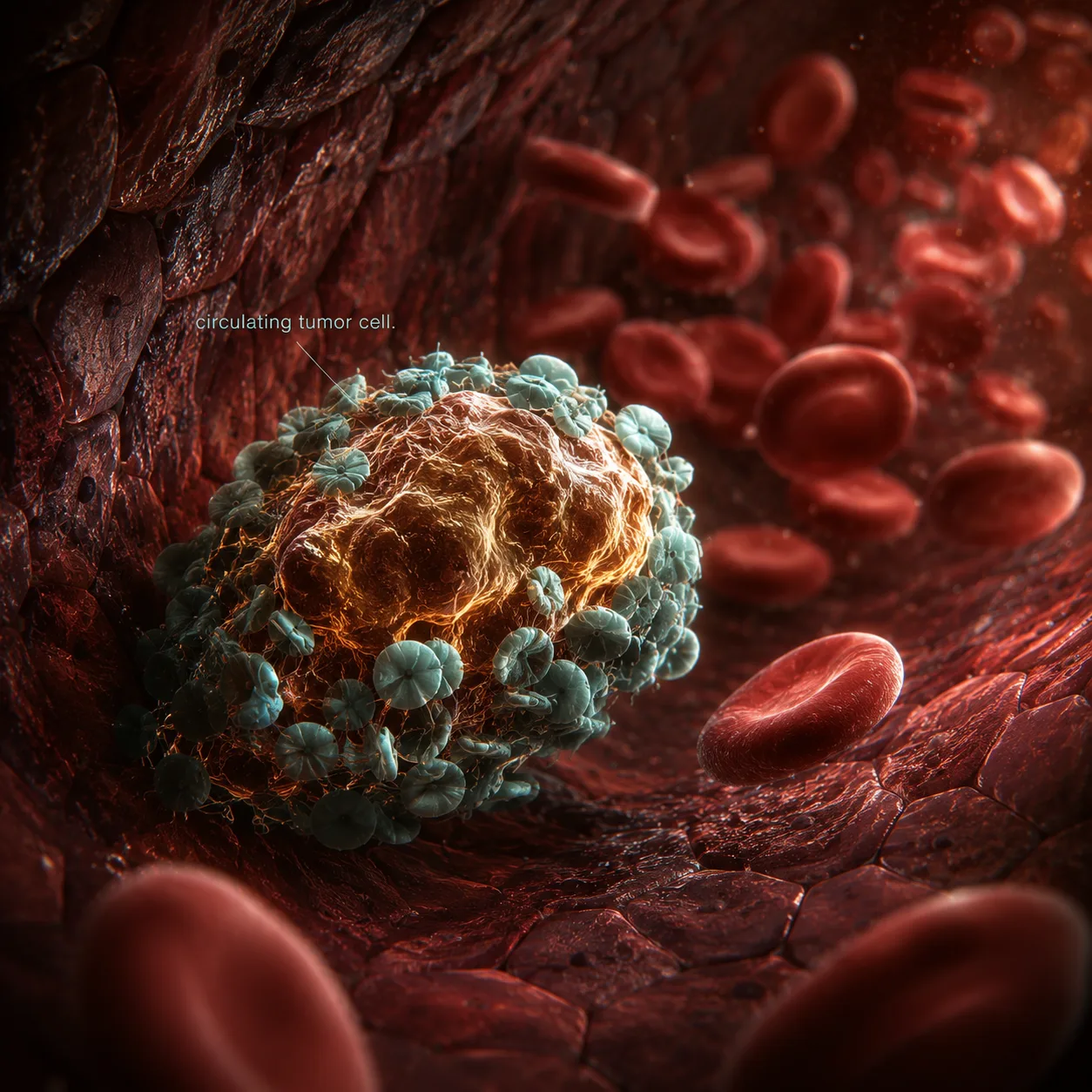
The bloodstream is hostile. Circulating tumor cells (CTCs) face:
- Shear stress from blood flow
- Anoikis from loss of matrix attachment
- NK cell killing — natural killer cells patrol the vasculature and efficiently eliminate most CTCs
CTCs survive by clustering with platelets, which physically shield them from shear stress and NK cells, and by activating survival signals that suppress anoikis. Platelet-CTC clusters are also better at extravasating than single CTCs, and platelet activation deposits fibrin around CTCs, creating a protective coat.
Step 5: Extravasation and colonization
Exiting a vessel at a distant site involves attaching to the endothelium, inducing endothelial retraction, and migrating into the tissue. Some CTCs exploit the same machinery as immune cells — expressing selectin ligands to roll along endothelium and integrins to arrest and transmigrate.
Colonization is where most attempts fail. A cell that successfully extravasates into liver or lung tissue is in a completely foreign microenvironment — different stromal cells, different growth factors, different physical matrix. The vast majority of extravasated cells die or enter a dormant state.
Definition(Metastatic dormancy)
A state in which disseminated tumor cells (DTCs) persist at distant sites without proliferating — sometimes for years or decades before emerging as overt metastases. Dormancy can be maintained by immune surveillance (immunological dormancy), by failure to activate angiogenesis at the new site, or by the new tissue microenvironment imposing growth arrest signals. Awakening from dormancy is poorly understood but has been associated with inflammation, tissue injury, and immune suppression.
Organotropism: why metastasis is not random
Cancer doesn't spread randomly. Breast cancer preferentially metastasizes to bone, lung, liver, and brain. Colorectal cancer goes almost exclusively to liver. Prostate cancer goes to bone. Melanoma goes to brain, lung, liver, and skin.
Stephen Paget described this in 1889 as the "seed and soil" hypothesis: the seed (metastatic cell) only grows in compatible soil (the right organ microenvironment).
The molecular basis for this organotropism involves:
- Chemokine gradients — cancer cells express receptors for chemokines concentrated in specific organs. Breast cancer cells frequently express CXCR4, whose ligand CXCL12 is highly expressed in bone marrow, lung, and lymph nodes.
- Exosome pre-conditioning — tumors secrete exosomes that travel ahead of CTCs to distant organs and reprogram the local microenvironment to be receptive. Pancreatic cancer exosomes specifically condition the liver; breast cancer exosomes condition the lung.
- Metabolic compatibility — the metabolic environment of the target organ must support the tumor cell's metabolic program. Bone metastases from breast cancer, for instance, exploit the bone remodeling cycle to access growth factors stored in the bone matrix.
Example(Bone metastasis and the vicious cycle)
In bone metastasis — common in breast, prostate, lung, and renal cancers — tumor cells secrete PTHrP (parathyroid hormone-related protein), which activates osteoclasts (bone-resorbing cells). Osteoclast activity releases TGF-β and IGF stored in the bone matrix, which in turn stimulates the tumor cells to secrete more PTHrP. This self-amplifying loop — the "vicious cycle" of bone metastasis — progressively destroys bone while fueling tumor growth. Bisphosphonates and denosumab (anti-RANKL) interrupt this cycle by targeting osteoclast activity.
Why metastasis is so hard to treat
Metastatic disease is harder to treat than primary disease for reasons beyond just spread. Metastatic cells have, by definition, passed through the bottleneck of the metastatic cascade — they are the survivors of a highly selective process. They tend to:
- Be more genetically diverse than the primary tumor
- Have active EMT programs that confer stem-like, therapy-resistant properties
- Sit in microenvironments (bone, brain) that are pharmacologically privileged — hard for drugs to penetrate
- Be in dormancy, where they're not actively cycling and thus not sensitive to anti-proliferative therapies
The challenge of treating metastatic disease is partly biological and partly a consequence of selection: the cells that metastasize are, almost by definition, the most fit and most resistant.
Summary(Summary)
Metastasis is a multi-step cascade — invasion through basement membrane, EMT, intravasation, survival in circulation (aided by platelet clustering), extravasation, and colonization — each step a bottleneck that eliminates most candidates. The fraction of tumor cells that complete the cascade is tiny but sufficient, given the scale of cell shedding from large tumors. Metastatic spread is not random: organotropism is determined by chemokine receptor-ligand compatibility, exosome pre-conditioning of target organs, and metabolic compatibility. The cells that successfully metastasize are a highly selected subset with stem-like, therapy-resistant properties — which is why metastatic disease remains the dominant cause of cancer mortality and the most challenging therapeutic frontier.